April 9, 2026
Webinar: Warning Signs, Risk Factors, and Strategies for Supporting College Students with Suicidality
Written by Guest Author
Posted in Depression, Emotional & Mental Health, Self Help / Personal Development, Webinars and with tags: mental health challenges, self improvement, suicide

College is supposed to be exciting. A fresh start. New friendships. Big dreams.
But for many students — and the people who love them — it can quietly become something else entirely.
Behind dorm room doors and glowing laptop screens at 2 a.m., there are students who feel deeply alone. Students who are overwhelmed by academic pressure, financial stress, social comparison, identity struggles, and the heavy weight of expectations. Students who begin to wonder if they matter. Those who feel so isolated and unloved that they may be tempted to end their own lives.
If you are a college student, you may recognize this feeling.
>If you’re a parent, you may fear it.
>And if you’re a faculty or staff member, you may worry you’ll miss the signs.
And that fear — the not knowing — can feel paralyzing.
The Silent Crisis on Campus
Undergraduate years are often portrayed as the “best years of your life.” But for many, they are some of the most emotionally intense years they will ever experience.
Students face:
- Academic rigor that feels relentless
- Pressure to succeed and define their future
- Loneliness in the middle of crowded campuses
- Financial stress
- Relationship challenges
- Mental health struggles that may surface for the first time
When these challenges compound, a student can begin to feel hopeless. And hopelessness, when left unaddressed, can become dangerous.
The cost of ignoring these realities is heartbreaking. At worst, it can mean death by suicide. At best, it can mean years of silent suffering, isolation, and preventable mental health struggles.
But there is another path.
What If We Were Prepared?
What if students walked onto campus equipped not only with a class schedule, but with tools for emotional survival?
And what if parents understood the warning signs and knew how to respond without panic or shame?
What if professors, advisors, and staff felt confident in their role as gatekeepers — able to recognize risk factors and intervene realistically and compassionately?
This is exactly what “Warning Signs, Risk Factors, and Strategies for Supporting College Students with Suicidality” is designed to address.
This focused webinar helps undergraduate students, prospective students, parents, and higher education professionals understand the risk factors and warning signs of suicidality among college students — and, just as importantly, how to realistically intervene.
You won’t leave feeling overwhelmed.
You’ll leave feeling equipped.
What You’ll Gain from Attending
By participating in this event, you will:
- Learn the warning signs and risk factors of potential suicidality on college campuses
- Understand your role as a suicide gatekeeper within your community
- Gain practical knowledge on how to intervene when concerns arise
- Become familiar with national and local suicide prevention resources
- Feel more confident having difficult — and life-saving — conversations
Knowledge replaces helplessness with action.
Preparation replaces fear with clarity.
And sometimes, one informed conversation can change — or save — a life.
Meet Your Presenter: Joey Harmon
Joey Harmon earned his Master’s of Science in Clinical Mental Health Counseling from the University of North Texas, a CACREP-accredited institution. He is a National Certified Counselor with the National Board of Certified Counselors, a Licensed Professional Counselor in Texas, and a Registered Telehealth Provider in Florida.
Mr. Harmon works with clients across the lifespan — including children, pre-adolescents, teenagers, and adults — and is trained in Acceptance and Commitment Therapy (ACT), Child-Centered Play Therapy, Child-Parent Relationship Training, Trauma and Grief Component Therapy for Adolescents, and Brainspotting.
Importantly, he brings extensive experience working directly with undergraduate populations. He served students at the University of North Texas through roles with the Center for Leadership & Service and the Student Money Management Center, provided counseling services to UNT students during his master’s practicum, and has continued working with collegiate populations throughout his career. He also currently serves on the advisory board for the HCU chapter of Phi Kappa Psi, mentoring and supporting undergraduate members in leadership development and mental health awareness.
This is not a theoretical presentation.
It’s grounded in real experience with real students.
You Don’t Have to Navigate This Alone
Whether you are preparing to enter college, currently in the middle of it, parenting through it, or serving students professionally, you deserve guidance, clarity, and tools.
The reality of suicidality on college campuses is heavy.
But silence and avoidance make it heavier.
Education creates hope.
Preparation creates protection.
Conversation creates connection.
If this topic touches your heart — or keeps you up at night — this webinar is for you.
Watch a replay of the presentation here.
This month’s webinar is titled Warning Signs, Risk Factors, and Strategies for Supporting College Students with Suicidality. It is facilitated by Joey Harmon.
He holds a Master of Science in Clinical Mental Health Counseling from the University of North Texas, a CACREP-accredited institution. In addition, he is a National Certified Counselor with the National Board of Certified Counselors. He is a Licensed Professional Counselor in the state of Texas and a Registered Telehealth Provider in the state of Florida.
We are going to be covering a subject that carries a great deal of weight, and we will speak more to that later on. This presentation is a slight variation of one that was provided in January at the Phi Kappa Psi Houston Alumni Association undergraduate leadership workshop, where various undergraduates of the fraternity Phi Psi gathered at HCU to learn different leadership skills. There, we had the privilege of speaking about suicidality in the context of fraternity chapters and what undergraduate leaders can do within their chapters to help improve the mental health of their brothers.
Goal
We are using that presentation as a template, but we are expanding the scope to focus on undergraduate college students in general. Our goal is to provide a general suicide awareness and response training while also highlighting unique factors for undergraduate populations, including specific risk factors, stressors, and protective factors, which we will conclude with tonight.
So we definitely want to end on a positive note for tonight, but we want to teach y’all the risk factors and warning signs of potential suicidality. We want to emphasize the gatekeeping nature of y’all, and we’ll get to what that means within the context of suicide later on in this presentation. We also want to familiarize y’all with different resources that y’all can refer people to if someone is feeling suicidal, should you find yourself encountering someone who fits that description.
The intention for this is broad. This can be useful if you are already a college student, if you are a high school senior or junior getting ready for college, if you are a parent of a college student or soon-to-be college student, if you work at a college or university and serve undergraduate populations, or if you simply interact with the collegiate population in general.
Our intention for this audience is to be as wide as possible, because just about everybody interacts with college students in some capacity, some a little more than others. But again, this also has a lot of great material for if you encounter anybody else who is struggling with suicide.
Stigmatized Topic
This is going to be a heavy topic. We know it is a guarantee that at least one person who is watching this video or joining us tonight has encountered suicidality in some capacity, whether it’s something you’ve personally struggled with, or whether you’ve been impacted by a loved one following through with suicide, or if a loved one has been suicidal in the past or is a survivor of suicide loss.
When someone completes suicide, it creates a crater. Think of a meteor or asteroid hitting a planetary body, causing a large crater, debris to fly everywhere, and a shockwave.
That’s what happens every single time a suicide happens, and many people are impacted by it. So we don’t want to shock-and-awe. It’s something we unfortunately see done in some trainings, but we are not going to get graphic.
We are not going to try to emotionally manipulate anybody. That would be incredibly irresponsible and morally wrong. We do want to go over some of the realities, though, because this topic cannot be done justice if we try to walk on eggshells around it. So we want y’all to be mindful of what comes up for you tonight.
We are not going to get more graphic than necessary. The goal here is to set you up with confidence and success so you can help somebody if they find themselves in this situation. We hope you never need to use these skills. We hope you never need to. But if you do, we want you to be prepared.
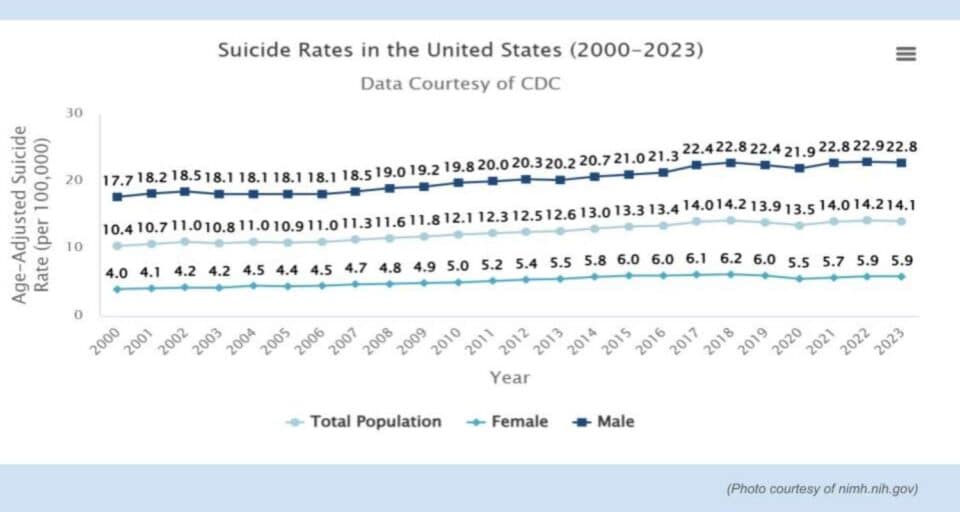
Suicide Stats
- Suicide was the 10th leading cause of death overall in the U.S. in 2024.
- For both males and females aged 18-22, suicide rose to the 2nd highest cause of death.
- (Center for Disease Control, 2024)
We are going to start with background on suicide, the suicide epidemic, and how it can impact college students specifically.
As of 2024, suicide is the 10th leading cause of death overall in the United States.
When this presentation was given in January, the 2023 numbers placed it at 11th. According to the Centers for Disease Control, that number went from 11th to 10th in just one year. And for those assigned male at birth or assigned female at birth within the traditional collegiate age range of 18 to 22, death by suicide rises to the second leading cause of death.
It is important to note that not everyone aged 18 to 22 is in college, and college students are not always within that exact age range. College is not for everybody, and there are many non-traditional students as well. So this is not a catch-all. But in the United States, a large proportion of undergraduate students do fall within this range, which is why we are using it as a reference point.
We also see, unfortunately, that this number has continued to rise over time, with small decreases at points but an overall upward trend.
We also want to address sex differences briefly. Among women and girls, suicide attempts are more frequent, often through less immediately lethal means, such as medication overdose. These situations are always serious and must be treated with urgency.
Research and data suggest that these attempts can sometimes reflect a cry for help or an expression of distress that has not been effectively communicated or heard. That does not apply universally, and we do not want to overgeneralize.
Typically, for men and boys, it is usually not an attempt. It is usually the case that if a man or boy is trying to kill himself, it is because he has already made it up in his mind to go ahead and do so. So women and girls attempt more than men and boys, but men and boys will typically complete suicide more than women and girls by using more lethal means and being more, we suppose, intentional, if you will, about it. This is not to be disparaging towards anybody, obviously, or to take an ounce away from any of that. We just wanted to give a little bit of context.
But no matter what, we see this rise here. And we also see a great number of people who are contemplating, making plans for, and attempting to follow through with suicide. We include this infographic here, also shared by the Centers for Disease Control. And the biggest thing we want people to take away from this is that these numbers are not accurate.
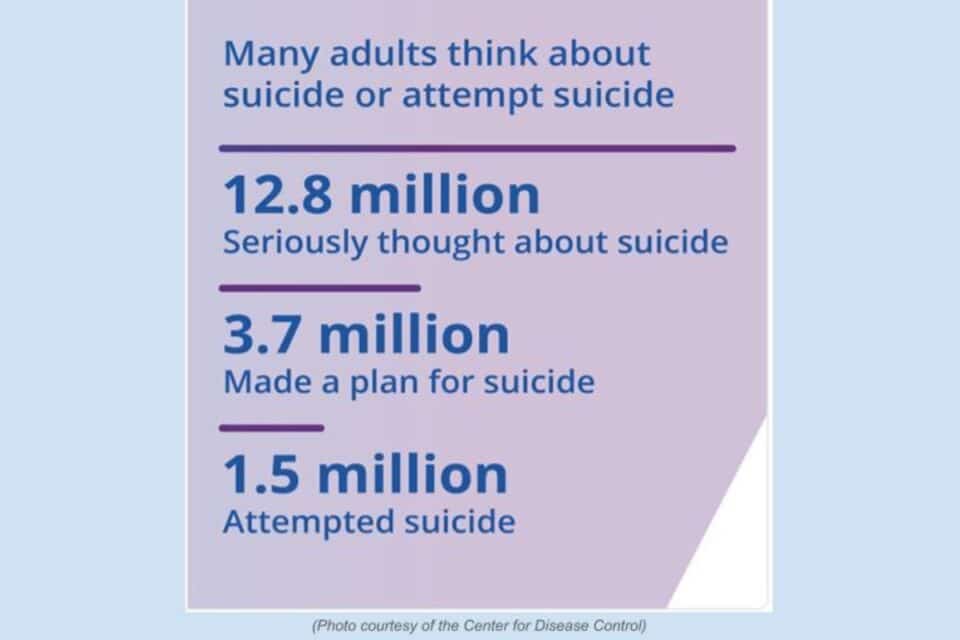
These numbers are lower than what the actual numbers are.
Because we note that this is a very stigmatized topic. Not everybody who thinks about, plans for, or attempts suicide is always going to talk about it with people. And even if they do, it is usually going to be a small handful of people, a small group of loved ones that they really trust, and that is who they are going to talk about it with.
When the CDC conducts surveys, they usually cold call. And it is understandable why, if someone was struggling with suicidality, they would not just admit that to a stranger calling them over the phone who allegedly is with the CDC. So we emphasize this to increase understanding of why people will not necessarily report if they are thinking about it, if they have planned it, or if they have attempted and survived. So these are the official numbers. The numbers in reality are bigger.
We are mentioning this info, not to shock and awe, but to encourage people to raise their eyebrows and keep their eyes wide open about the reality of this epidemic.
Collegiate Suicide Risks
Moving into particular concerns for the collegiate population, as those who have gone to college, are currently going through college, or are getting ready for college, there are things that the undergraduate population has to face that can be quite harrowing, especially if they have to be away from home for the first time and are not commuting.
That could be a different city, a different state, a different nation, or even a different continent. International students, in particular, have to go through a great deal.
And there is also the challenge of not having as close contact with high school friends, the same people they were forced to see day in and day out, sometimes for longer than four years. People do not necessarily go to the same college, and that creates a unique stressor. There are increased academic stressors, and there is also increased pressure to get life figured out.
As a culture, there is often an implicit or explicit message communicated to teenagers that when they are 17 or 18 and start applying for college, they need to know what major they are going to pursue, stick with that major permanently, and stick with that career permanently, and that this is what they do until they retire or die.
Not everyone is explicitly saying those things, although unfortunately some people do state that directly to high school students. However, the implicit message is usually clear. As a result, many students entering college may not realize that switching majors is a completely viable option. They do not have to stay with the same field they selected when they applied for admission at 18.
Even after graduating with a particular degree, they do not have to remain within that field. They can use their degree in a wide range of other fields and in different ways, but that message is not always clearly communicated. This can increase pressure to feel like everything must be figured out immediately. There can be a strong sense that you need to achieve the highest possible grades to remain competitive in the job market.
There are also increased risks related to substance use and misuse in college environments.
College party culture is a well-known factor in this context. Additionally, when individuals turn 21, they are legally able to consume alcohol, and in some cases, depending on state laws, to use tobacco products, and in certain states to use THC legally.
Or if they have a friend who is old enough, or access to a convincing fake ID, they may gain access to a wide range of different substances. Parents often have significantly less oversight at this stage. Combined with increased stress and peer pressure, this can create a recipe for disaster.
As a result, college students often face a unique set of risks that can negatively affect mental health, which may unfortunately contribute to increased suicidality. There is also a need to pause on the role of parenting before moving on. Although this is not a parenting presentation, there are two extremes that parents can take when raising children.
On one end, in more permissive households, students who go off to college—especially those living on campus or away from home—may not have developed the same level of self-reliance or independence as peers who were expected to complete chores, manage homework, or study independently.
This can lead to a sharp sense of incompetence, feelings of worthlessness, or at the very least feeling unprepared, as well as possible resentment toward parents. There can also be embarrassment about having to figure things out at a later stage than might have been more developmentally helpful.
On the opposite end, an authoritarian parenting style may result in college students not viewing their mother, father, or both parents as safe emotional supports. In cases where there has been abuse or severe rigidity, there are often additional reasons why parents are not seen as emotionally safe.
In these situations, students may not have been equipped with as much support in developing emotional intelligence and an emotional sense of endurance and resilience.
With these factors combined, the goal is to aim for a middle ground—authoritative. We are moving on from this topic, but with those factors plus the particular and unique stressors, it becomes especially difficult for students. It becomes very difficult for students, particularly with the existential concerns that were discussed earlier.
Again, this is not presented to shock and awe, but to raise awareness. So the picture may show statistics such as the 10th leading cause of death in the US, the 2nd leading cause of death for 18 to 22-year-olds, and rising rates overall. College students, or peers who are also in college, may be going through a great deal. The question then becomes what is to be done.
The intention is to liberate people from feeling as if the weight of the world is on their shoulders. For those viewing the content or in the audience, the goal is not for them to feel as if they need to take on all of that burden.
The role is, in a sense, only to “gatekeep.”
In the context of suicidality, gatekeeping refers to those in close contact with members of their communities being able to identify warning signs, understand risk factors, ask appropriate questions, and refer individuals experiencing suicidal thoughts to appropriate resources and trained professionals who can take it from there.
In that sense, the role is more about passing the baton. Gatekeeping within suicide is more of a baton race. We are running the race for a short period of time and then handing it off to someone else. It is still not a perfect metaphor, and this will be addressed later on. There is still a role after referring someone to another person. However, the primary role is gatekeeping.
We are not crisis counselors, and that is not an expectation placed on us. There is no expectation to be trained in that capacity within the context of this presentation. The emphasis is that the role is only to gatekeep, and it can be a very effective intervention. A great deal can be done even with basic knowledge, even without a psychology background.
Common Warning Signs
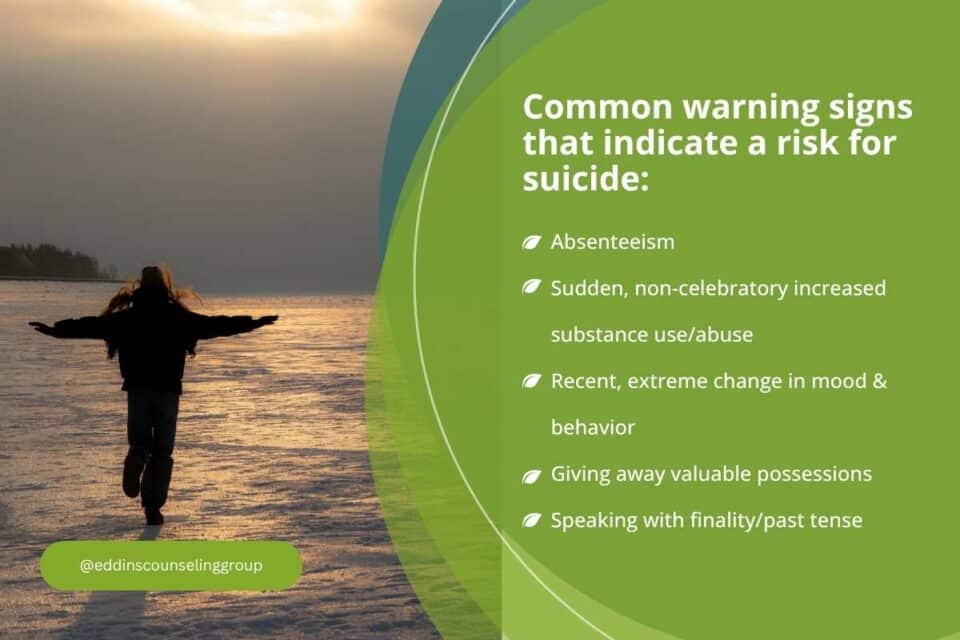
Specific actions that a person takes which indicate a higher likelihood/risk of suicide in the near future.
- Absenteeism
- Sudden, non-celebratory increased substance use/abuse
- Recent, extreme change in mood & behavior
- Giving away valuable possessions
- Speaking with finality/past tense; “You were always so kind to me.” (Varshney et al., 2024)
Moving into warning signs, a warning sign refers to a direct behavior. It is an observable action that can be witnessed in someone that may indicate possible suicidality, meaning the person may be considering suicide, may be at risk, or may have made a decision regarding suicide.
The list can be referenced, and time is being considered, so not every item is addressed in detail, with the exception of recent extreme changes in mood and behavior. This can also apply in a positive direction. If someone has a sudden increase in positive emotions and becomes unusually friendly out of nowhere, especially if that is not consistent with their prior behavior, that can be a warning sign.
When preparing to leave a party, event, or function, and the decision has already been made to go home, people often go around to others, smile, hug, shake hands, and express how good it was to see them, with plans to meet again. Friendliness increases because the decision to leave has already been made.
In some cases, individuals who are experiencing suicidality may show similar patterns. They may have decided to end their lives and begin saying their goodbyes. This can also connect to behaviors such as giving away valuable possessions and speaking with finality.
It is also emphasized that no single sign should be interpreted in isolation as definitive evidence of suicidality.
For example, if Johnny was not in calculus today, that may mean many things. It could simply mean he was sick. At a formal event with a friend for an organization, there may be a wistful moment where someone says they have always been really grateful and have always appreciated the other person. That is not necessarily the moment to begin asking questions about suicide in that context.
Any of these signs individually are not necessarily indicators of risk for suicide, but they need to be considered in combination. We need to stay aware of patterns and ask whether multiple indicators are present at the same time. For example, Johnny may not have been showing up to class for a while, may be using alcohol when preparing to leave his dorm, may be giving away valued possessions such as a vinyl collection, and may be making statements such as “It will all be over soon.”
In situations like that, there is a clearer pattern where concern becomes more warranted, and questions may need to be asked. These are the common warning signs. The expectation is to be aware of them and to understand how they can appear in combination rather than in isolation.
3 Key Risk Factors for Suicide
- Unloveable
- Unsolvable
- Unbearable
(Rudd & Bryan, 2021)
Heightened by any history of abuse/neglect, prior history of suicide attempts, and/or acute & intense stress.
Moving from warning signs to risk factors, risk factors refer more to a person’s emotional state, but especially their history and background—factors that increase overall vulnerability. An example is that a person is at increased risk for lung cancer if they are smoking two packs a day; in a similar way, certain experiences or conditions increase risk for other outcomes.
The risk factors listed above are referenced, and while there was an initial intent to go over several common ones, a few are highlighted instead. Dr. Rudd and his team at the University of Memphis have conducted important research into individuals who have survived suicide attempts and have contributed qualitative findings about what led to those experiences.
Three core themes emerged across survivors. One is feeling unlovable, which is not only the belief that no one loves the person, but also that there is an inherent deficit that makes them uniquely incapable of being loved—that no one could or would love them.
Another is the perception that one’s problems are unsolvable and unbearable, where the person feels unable to imagine a future in which they are no longer dealing with their current difficulties and cannot see a way out.
They believe that nobody cares. That is why we emphasize being incredibly supportive of the people around us, because no one can always know what another person is going through. No one can always know what someone else is experiencing.
We would say, in our view, that the first factor is by far the most important. This connects to later discussion about connection and how to follow up and be present for someone.
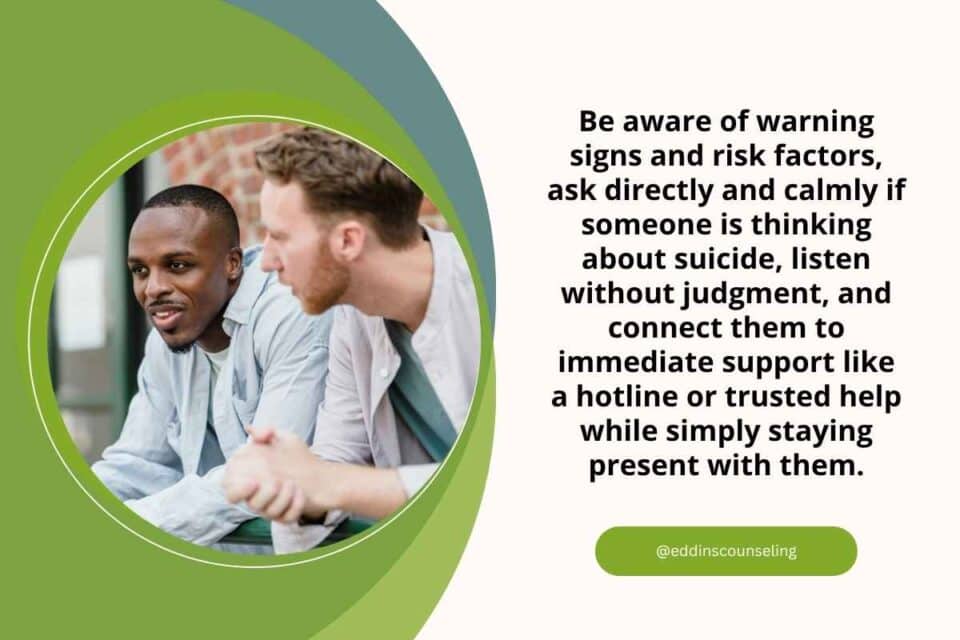
How to Intervene
- Be on the lookout for warning signs & risk factors.
- Ask directly if they’re thinking about killing themselves. Be direct.
- “I have some weird & heavy questions to ask you, but I’m asking them because I care about you.”
- Thinking, wanting, planning, access, attempted
- Be non-judgemental, keep a level composure, and listen.
- Call 988 or another hotline (see next slide).
- Be there.
In terms of gatekeeping, it is possible to be highly effective in supporting and even saving a life, and being a positive force for someone without needing to do an excessive amount in the moment.
The key point is to be aware of warning signs and risk factors. We also pause to emphasize one important point: there is a need to ask directly, “Are you thinking about killing yourself?” We stress that the question must be direct, even though it will likely feel uncomfortable and unfamiliar.
There is a reason for this directness. This is an area where there cannot be ambiguity or “gray area,” because the stakes are high. There is little room for uncertainty in matters of suicide risk. Because of this, we emphasize being direct rather than indirect or vague.
We note that questions such as “Do you just not want to be here anymore?” or “Do you wish your problems would go away?” are too ambiguous. Instead, it is important not to avoid the topic or speak around it. At the same time, the approach should be nonjudgmental and relatively calm. “Casual” in this context does not mean joking, dismissive, or irreverent, but rather grounded and steady.
We also caution against being overly intense or dramatic, as that can increase discomfort or shame for the person involved, which is counterproductive.
The goal is to reduce shame, not increase it, for someone who may be experiencing suicidal thoughts.
We include an example of how we frame these questions with clients: we begin by warning that the questions may feel direct or intense, but that they are being asked out of care and concern. We then proceed with direct questions such as whether the person is thinking about suicide and whether they have any intent or plan.
If a person discloses details about access to potential means, such as methods involving self-harm or access to lethal tools like firearms, we would continue to ask clarifying, safety-focused questions about those specifics in a structured and careful way.
The emphasis is on not being flippant, dismissive, or overly casual.
At the same time, we need to avoid being overly tense or fearful when asking these questions. They should not come across as hesitant or “wobbly.” One additional benefit of asking directly in a calm, matter-of-fact way is that it can help reduce stigma. It can help the person feel that they are not being treated as “baffling,” but rather as someone being spoken to in a straightforward, normal way. That shift alone can reduce shame and make it easier for the person to talk.
The key questions are important to capture clearly. These include asking directly: “Are you thinking about killing yourself?” and “Do you want to kill yourself?” They also include asking about intent and plans, such as “Do you have any plans to kill yourself?” and, if something has already been mentioned, following up with clarification like “Where does that live?” and asking about access.
It is also important to ask about history, such as whether they have attempted suicide in the past. The overall approach should remain nonjudgmental, with an emphasis on listening. The focus is on being present and truly listening, because the person may be sharing with someone who is the first to demonstrate genuine care not only by asking the questions but by staying engaged with their response.
It is noted that, for some individuals, suicide attempts can occur in contexts where they have felt unheard or uncared for, and being listened to can be a meaningful protective factor. From there, the next step is referral to support resources such as 988 or another hotline. Support does not end at referral; it also includes follow-up and continued presence afterward.

There is a distinction between 988 and 911.
988 is the National Suicide and Crisis Lifeline. A key focus is addressing misconceptions about it. One common myth is that if someone is honest about suicidal thoughts, emergency services will automatically respond with police involvement or hospitalization. This is not an accurate generalization in modern practice.
Services like 988, coordinated through SAMHSA, prioritize minimizing intrusion into a person’s life as much as possible while still responding appropriately to the level of risk. The guiding principle is to be as minimally invasive as safety allows.
If the intensity is not present, then there is no need to involve emergency personnel or discuss hospitalization. In cases where someone is feeling overwhelmed but has not developed a plan or intent, and does not wish to act on suicidal thoughts, the appropriate response is to talk with them and provide support.
Most of the calls they get, they will talk to the person, help create a safety plan to keep them safe, offer a follow-up, and they will follow up, you know, maybe a day or so later, and then just keep in touch with them for a little bit to make sure things are good.
And try to plan for like, okay, who are some safe people that they can be around and talk to afterwards? So that’s what this first point is here for. These are kind of the three different stages that they use at 988. A lot of the time, we just talk to somebody on the phone.
This could be if they are suicidal or contemplating self-harm, or if they are with somebody and don’t know how to go about helping them, they can also call 988, and they will coach them through it or ask if they can hand the phone over to us.
The second level is the crisis mobile response team.
That’s where they will send one or two people over in person to talk to the individual and basically do the same thing here. But then that team will also leave without the person. And again, the goal is to be as minimally invasive as possible so as not to swat a fly with an ax.
They don’t want to be so heavy-handed that the mental health situation worsens for the person. And that’s the last thing any of us want. Again, we don’t want to produce shame or increase any shame with this. We want safety to be number one.
Safety is number one, no matter what, no matter how they feel about us. It’s better that they hate us if it means they are safe. We want to keep shame levels in mind, but we have to keep their safety as the number one priority. But right next to that is shame.
We want to decrease shame.
We don’t want to bring about shame. And neither do we at SAMHSA, nor does 988. So they might send a team over to help them out, but then they leave. And obviously, if the intensity is there, if the intensity requires it, they will look into temporary hospitalization or stabilization facilities.
But even then, they try to keep the person there for only as long as they need. Just until they are no longer a threat to themselves or anybody else going forward. So they try to walk this line where they don’t want to be dismissive toward the intensity in the moment. They don’t want to just have a phone call if it seems like there is a very imminent danger. Maybe they are in the midst of something.
But they also don’t want to send a team over because someone is having a rough day, has not contemplated it in the past, and is experiencing some mild ideation. That’s something they can handle via a phone call.
So we say all this to try to demystify and bring some clarity to what 988 is, its utility, and its effectiveness in helping people.
Follow Up
Follow-up is crucial.
When we help somebody in any capacity, whether they are feeling suicidal or not, we are providing evidence that we care, but we need to show proof that we care. There is a difference between evidence and proof. We have shown evidence, but we need to prove it by continuing to be a present force in the person’s life, in the student’s life afterward.
So if they are involved in a bunch of different extracurricular activities, maybe they do not need to be an officer temporarily in their organization. Maybe they do not need to go to all these different events, or at least plan all these different events. But we encourage them to still be in contact with the people they trust.
Even if those are friends they have not opened up to about this. The more they can be around those who care about them and want to see them again, the more those thoughts that nobody cares about them can be dispelled.
By being present with them and also asking candidly about the topic of suicide and their history of suicidal thoughts, we can say, “Hey, we just wanted to check in on the suicidal thoughts and see how you’re doing with that.”
That can reduce stigma. Because again, we’re emphasizing implicitly that they’re not baffling. They’re going through a lot, and their brain jumped to a conclusion to try to make their pain go away.
They’re not baffling. They just don’t want to put up with what they’re going through right now. And we care about them and don’t see them as a quote-unquote baffling person. We’re here for them. And we continue to be there.
Now, we don’t want to overwhelm them. We don’t need to be mother hens about it. That creates its own issues. We don’t want to be helicopter or lawnmower parents. We also don’t want to overdo it because that can induce shame.
If we’re calling all the time, if we’re texting all the time, if we sound nervous whenever we talk to them. They’re going to pick up on what’s not being said, and they’re not going to want to interact with us that much.
So we want to strike that fine balance between still being a present force in their life, not talking about it all the time, but checking in on them every once in a while just to see how they’re doing. And like we said, we prove it by giving our presence.
We know that sounds cheesy, but really, that shows a lot. It proves that, no, we do care about them and they are not, in fact, unlovable. There are people who do love them and want to see them continue to succeed and to see them show up the following day and the day after that and the day after that and so on and so forth, and the year after that, the decade after that, and beyond.
Unique Protective Factors for College Students
- More people & opportunities to help provide belonging & meaning, such as spiritual groups, Greek Life, political organizations, athletic teams, etc.
- Larger access to mental health resources.
- Rising awareness about mental health needs on college campuses.
To end on a more hopeful note, there are unique protective factors for our college students. Quite frankly, being in college means that they have access to a whole sea of different opportunities to make connections with other people.
Some of the closest friends we have, we personally met in college. We were able to meet our spouses because of college connections and the people we were able to meet through those experiences. And so, with the large number of different kinds of organizations that are present, it helps a person—it can help a college student feel more connected with people and find a deeper sense of meaning and belonging.
Whether it’s through any of these organizations or others that we haven’t listed here, any kind of special interest group, just anything that helps reaffirm that they have a direction they can move their life toward.
They have something bigger than themselves to dedicate themselves to. They have people along the way who are willing to help them and whom they can get along with.
College students have greater access to mental health resources now more than ever on their campuses.
Any college campus is going to have its own counseling team, and that is because of a rising awareness of the importance of mental health on our universities, thankfully.
Now, we also do not want to look at this through sunshine-and-rainbows, rose-colored glasses. It is not as if all college counseling departments are created equal, unfortunately. But that being said, they’re there when that didn’t used to be the case even a couple of decades ago.
There’s less stigma surrounding that. And even if a college’s counseling department is booked full for the semester, they can always refer a student to different clinics within the community. So there is always going to be a resource for them.
And a lot of us who have worked in higher education—as graduate assistants or in other roles—have seen all kinds of trainings and awareness initiatives taking place to help make sure everybody understands the importance of mental health for our students and their lives and families.
So thankfully, it’s kind of a rising tide that floats all boats. But the biggest thing to take away is the unique sense of connection that someone attending college has the opportunity to pursue.
Other Hotlines/Resources
On that hopeful note, we wanted to end by going over a couple of different resources.
- National Suicide Textline: Text TALK to 741-741
- The Trevor Project: Call 1-866-488-7386 or text START to 678-678
- Local on-campus counselors/resources
- Local county’s mental health response team
- The QPR Institute
So 988 is obviously the National Suicide Hotline. It is also a text line, and we believe you can text 988 as well. Another national crisis text line allows individuals to text TALK to 741741.
The Trevor Project is a wonderful organization that specifically helps members of the LGBT community. We believe it is focused primarily on queer youth, though we could be mistaken about the youth component. For members of the queer community who are struggling with any kind of mental health crisis (especially self-harm or suicidal thoughts) you can call the number on the screen or text START to 678678. It’s a really easy number to remember.
Of course, since we’re talking about colleges, there are also on-campus counselors and resources. As we said, if those services are full or if students do not feel comfortable using them, those offices can always refer students elsewhere. They can provide information about different clinics within the community.
Any local county is also likely to have a mental health response team available if needed.
And finally, we want to give a shout-out to the QPR Institute. QPR stands for Question, Persuade, Refer. They provide training very similar to what we’ve discussed today. They cover many of the same topics, though they may use different terminology or emphasize different aspects.
More training is always better than less. They also offer specialized training opportunities. As of now, they are offering training for professionals who serve youth and work with youth. That may or may not include individuals within the traditional 18-to-22-year-old college-age range.
It is usually geared toward younger children. But still, they offer different kinds of training for different populations all the time, as well as our general training, which is very, very good. So we want to give the QPR Institute a shout-out as well.
References
Here are our references for the evening.
- Center for Disease Control. (2024)
- WISQARS Leading Causes of Death Visualization Tool
- Mental Health Services Administration. (2020).
- National Guidelines for Behavioral Health Crisis Care Best Practice Toolkit.
- Rudd, M.D., & Bryan, C.J. (2021). The Brief Suicide Cognitions Scale: Development and Clinical Application. Frontiers in Psychiatry, 12, 1-10.
- Varshney, K., Patel, H., & Mansoor, A. P. (2024). Risks and Warning Signs for Medical Student Suicide Mortality: A Systematic Review. Archives of Suicide Research, 28(4), 1058-1076.
- Washburn, C. A., & Mandrusiak, M. (2010). Campus Suicide Prevention and Intervention: Putting Best Practice Policy into Action. Canadian Journal of Higher Education, 40(1), 109-119.
Feel free to visit additional resources:
1. Articles on specific topics on our blog.
2. RSVP for one of our free monthly webinars (or view past webinars)
3. Follow us on Facebook and Instagram for additional interviews and tips
4. Take another one of our self-test quizzes
5. Schedule a consult and find out how we can support you.
If you have any questions, you can always get in contact with us for any kind of follow-up or additional information. If you’re interested in any of our services at Eddins Counseling Group, we have a couple of locations in Houston—one in the Heights right off T.C. Jester and one in Montrose on West Alabama.
We offer in-person and virtual counseling and therapy services, play therapy, career counseling, trauma-informed therapy, EMDR, Brainspotting, and many other services.
Feeling overwhelmed, unsure how to respond to someone in crisis, or concerned about suicidality in yourself or someone else? These situations are real and can feel confusing and heavy, and knowing how to respond can make a meaningful difference. By learning how to recognize warning signs, respond with care, and connect people to appropriate levels of support, we can help protect safety while also reducing shame and stigma.
If you’re ready to learn more about supporting someone through suicidal thoughts or navigating crisis situations, our therapists are here to help. To begin, give us a call at 832-559-2622 or schedule an appointment online. We also offer online therapy for added convenience and flexibility.